


{kind=link}
{kind=link}
-

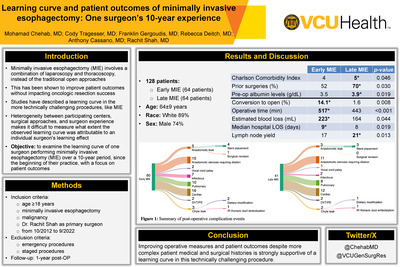
Learning curve and patient outcomes of minimally invasive esophagectomy: One surgeon’s 10-year experience
Moamad Chehab M.D., Cody Tragesser M.D, Franklin Geroudis M.D., Rebecca Deitch M.D., Anthony Cassano M.D., and Rachit Shah M.D.
Objective: To examine the learning curve of one surgeon performing minimally invasive esophagectomy (MIE) over a 10-year period since the beginning of their practice with a focus on patient outcomes. Methods: This is a retrospective study of all patients undergoing MIE for malignancy by one surgeon at an academic high-volume tertiary center over a 10-year period (10/2012 to 9/2022). Patients were stratified into 2 equal groups based on chronological order and termed Early MIE and Late MIE. Primary outcomes included operative measures and patient outcomes over a 1- year period post-operatively. Results: A total of 128 patients were identified, divided into Early MIE (64 patients) and Late MIE (64 patients). Mean age was 64±9 years, with a majority of white (114 [89%]), male (95 [74%]) patients who received neoadjuvant chemoradiation therapy (98 [77%]). Patients in the Late MIE group had higher median Charlson Comorbidity Index (5 vs 4; p=0.046), more prior chest and/or abdominal surgeries (45 [70%] vs 33 [52%]); p=0.030), and higher mean preoperative albumin levels (3.9 vs 3.5; p=0.019). More patients in the Early MIE group had conversion to open procedure (9 [14.1%] vs 1 [1.6%]; p=0.008). Comparing Early MIE vs Late MIE, mean operative time was 517 vs 443 minutes (p< 0.001), estimated blood loss was 223 vs 164 cc (p=0.044), and median hospital stay was 9 vs 8 days (p=0.019). All resections had negative margins confirmed on frozen sections, with higher lymph node yield in the Late MIE group (21 vs 17; p=0.013). Figure 1 is a summary of post-operative complication events. Conclusions: Improving operative measures and patient outcomes despite more complex patient medical and surgical histories is strongly supportive of a learning curve in this technically challenging procedure.
-

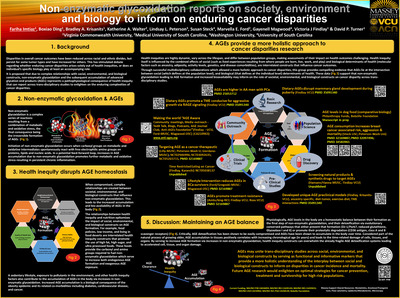
Non-enzymatic glycoxidation reports on society, environment and biology to inform on enduring cancer disparities
Fariha Imtiaz, Boxiao Ding, Bradley A. Krisanits, Katherine A. Walter, Lindsay L. Peterson, Susan Steck, Marvella E. Ford, Gayenell Magwood, Victoria J. Findlay, and David Turner
Background: Despite advancements in cancer treatment, disparities in incidence and mortality persist among different races and ethnicities. These disparities are influenced by an intricate interplay between environmental, biological and social factors that underscore the need for a multifaceted approach to understand this relationship. Objective/Aim: To show that advanced glycation end products (AGEs) due to non-enzymatic glycoxidation represent informative and functional markers that report on the combined impact of environmental, biological and social factors on enduring cancer disparities. Methods: To address this objective, a more holistic approach to disparities research was used ranging from basic research, population-based investigations, preclinical and clinical studies, as well as initiatives aimed at raising community awareness. Results: In first of kind in vitro, ex vivo, and in vivo basic studies, dietary AGEs were shown to exacerbate metabolic, immune and oxidative dysfunction within the breast and prostate tumor microenvironment (TME), to promote aggressive tumor growth through their interaction with the receptor for AGE (RAGE). Complementary population-based studies, indicate that higher intake of dietary AGEs is positively associated with increased breast cancer risk in women. Postmenopausal women with high dietary AGE consumption were found to be at higher risk of advanced-staged tumors and postdiagnosis intake of dietary AGEs associated with increased mortality. Further supporting an oncogenic role for AGEs, high circuiting AGEs were also shown to correlate with a lower breast cancer metastatic free and recurrence free survival. Critically, pre- and clinical studies from the lab have shown that lifestyle intervention is a viable option to reduce AGE levels as well as AGE induced tumor growth. Based upon these and additional data, the labs community outreach program has been developed and is aimed to raise awareness about the role of AGEs in cancer and to promote lifestyle changes that can reduce AGE exposure. Conclusion: This research illustrates a novel integrated approach focused on AGE accumulation (informative marker) and pro-tumorigenic function (functional marker), for understanding and addressing the role of environmental, biological and social factors on enduring cancer disparities. Future AGE focused efforts aim to develop interventional and pharmacological strategies that can reduce the burden of cancer in vulnerable populations. These studies will integrate biosocial determinants to further investigate how AGEs contribute to cancer and to develop and refine prevention and treatment strategies across diverse populations.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.